|
||||||||||
Suction
Curettage Management
of Major Jones
Operation Richardson Composite Operation Total
Abdominal |
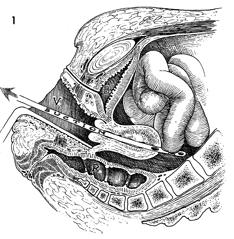
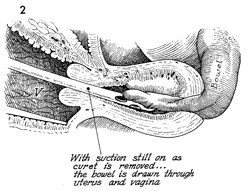
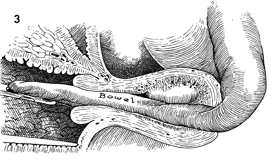
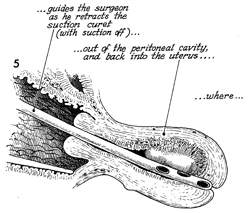
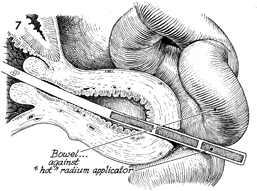
Management of Major Uterine Perforation of the uterus by the suction curettage cannula or by the tandem during radium application can cause serious complications of the small and large intestine if it is managed improperly. There is a distinct difference between the effects of these two kinds of perforation. If perforation occurs during suction curettage, the small bowel may be sucked into the eyes of the curet and pulled through the opening into the endometrial cavity and out through the cervix. Laceration of the small bowel can occur during this procedure. Although the large bowel is difficult to pull through the uterine perforation and out the cervix, the suction curet can attach itself to the wall of the large bowel and evulse a segment of it. A different problem exists with the intracavity radiation therapy radium tandem. If the tandem perforates the uterine wall and the perforation is not recognized, it may cause severe radiation damage to the small bowel on which it comes to rest. In both of the above situations, the
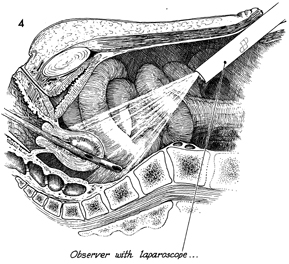
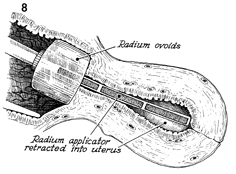
surgeon should immediately insert a laparoscope through the umbilicus
under direct vision withdraw the suction curet or the tandem back into
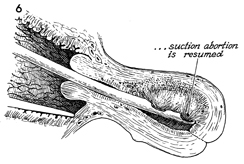
the uterus. In the case of the suction curet, the suction should be
reapplied, and the pregnancy should be completely terminated to avoid
further complicating the situation by adding the sequelae of incomplete
abortion. In cases of perforation by the radium tandem, once the tandem has been replaced back into the uterus, the radium application can be preceed, as indicated. Points of Caution. If perforation occurs during suction curettage, the suction should be turned off immediately to reduce the degree of injury to the intestine. Technique
|
|||||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.