|
||||
Suction
Curettage Management
of Major Jones
Operation Richardson Composite Operation Total
Abdominal |
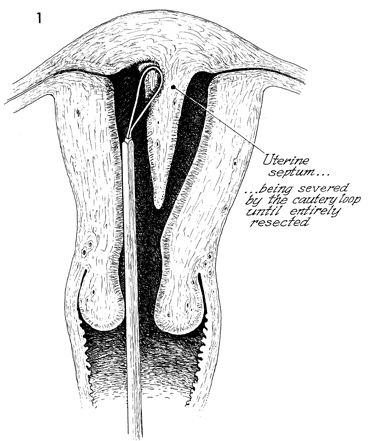
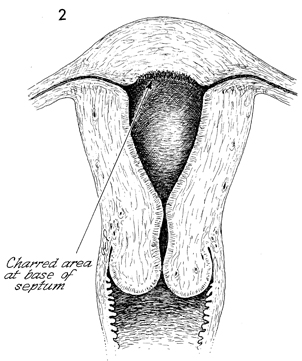
Hysteroscopic Septal Resection A patient who is unable to carry a pregnancy to term is sometimes found, on hysterosalpingogram, to have a septate form of double uterus. In such cases, resection of the septum often corrects the problem and results in a successful pregnancy. Before the introduction of the hysteroscopic operative instruments, this operation required a laparotomy as well as a hysterotomy with resection of the septum, i.e., Jones, Strassman, and Tompkins operations. The introduction of operative hysteroscopic instruments offers a new form of treatment that avoids a laparotomy, resulting in a shorter hospitalization and faster recovery. Physiologic Changes. A septate uterus is thought to cause fetal wastage because it cannot provide sufficient endometrium, which, in turn, provides nourishment for the developing placenta. When the septum has been removed, adequate endometrium returns, and nourishment becomes available. Points of Caution. Loop electrical excision can be associated with severe bleeding. Perforation of the uterus and injury to the adjacent intestine or bladder are possible but rare. Expansion of the endometrial cavity with 5% dextrose in Ringer's solution improves visualization and reduces hemorrhage, therefore allowing accurate loop electrical excision and electrocoagulation of vessels that are bleeding. Technique
|
|||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.